A dramatic case of Behçet disease successfully treated with infliximab

Main Content
A dramatic case of Behçet disease successfully treated with infliximab
Teresa Pinto-Almeida, Isabel Amorim, Rosário Alves, Manuela Selores
Dermatology Online Journal 19 (4): 18
Department of Dermatology, Centro Hospitalar do Porto – Hospital de Santo António, Porto, PortugalAbstract
Behçet disease is a chronic relapsing systemic disease with possible life-threatening presentations. Management of this disease can be challenging and reports of the off-label use of anti-TNFα agents for the treatment of severe manifestations are increasing, with good results. The authors report a case of Behçet disease with a sudden and severe multi-systemic onset successfully treated with infliximab.
Case report
A 34-year-old woman presented in our emergency department with a 1-week history of asymptomatic cutaneous lesions and one oral aphthous ulcer, together with fever and myalgia. She was otherwise healthy and was on no regular medication. There was no history of infections or drugs before the development of the cutaneous lesions and she denied similar previous episodes.
 |  |
| Figure 1 | Figure 2 |
|---|---|
| Figure 1. Clinical features of the sparse cutaneous lesions on the thorax and abdomen Figure 2. An erythematous pustule on the right upper back | |
 |  |
| Figure 3 | Figure 4 |
|---|---|
| Figure 3. Erythematous macules and papules on the lower back Figure 4. Cutaneous lesions on the lower limbs | |
 |
| Figure 5 |
|---|
| Figure 5. Clinical features of the aphthous ulcer on the upper lip |
Physical examination revealed erythematous papules and pustules. 2-8 mm, localized on the trunk and limbs and one aphthous ulcer on the upper lip, 6 mm in diameter. She was febrile (38°C) and there were no other findings on physical examination. Giving the systemic presentation, she was hospitalized for investigation.
 |  |
| Figure 6 | Figure 7 |
|---|---|
| Figure 6. Genital ulcer developing 2 days after the patient was hospitalized Figure 7. Two aphthous ulcers on the tongue, developing during hospitalization | |
 |  |
| Figure 8 | Figure 9 |
|---|---|
| Figure 8. Erythema nodosum-like lesions on the lower limbs Figure 9. Highlight of a cutaneous lesion on the thigh | |
Two days later she developed a painful genital ulcer and 2 new aphthous ulcers on the tongue. The cutaneous lesions on the lower limbs evolved to erythema nodosum-like nodules. She then developed intense headaches and impaired vision followed by paraparesis, left facial palsy, and loss of urinary sphincter control. At this point, she recalled having recurrent oral aphthous ulcers for the last 2 years, but had never considered them to be important. Laboratory workup disclosed leukocytosis (17.32 x 10³/µL, normal 4.00-11.00) with neutrophilia (11.74 x 10³/µL, normal 2.00-7.50) and elevated C reactive protein (144.02 mg/L, normal 0.0-5.0). Serologic and immunologic studies, blood, and urine cultures were negative.
 |  |
| Figure 10 | Figure 11 |
|---|---|
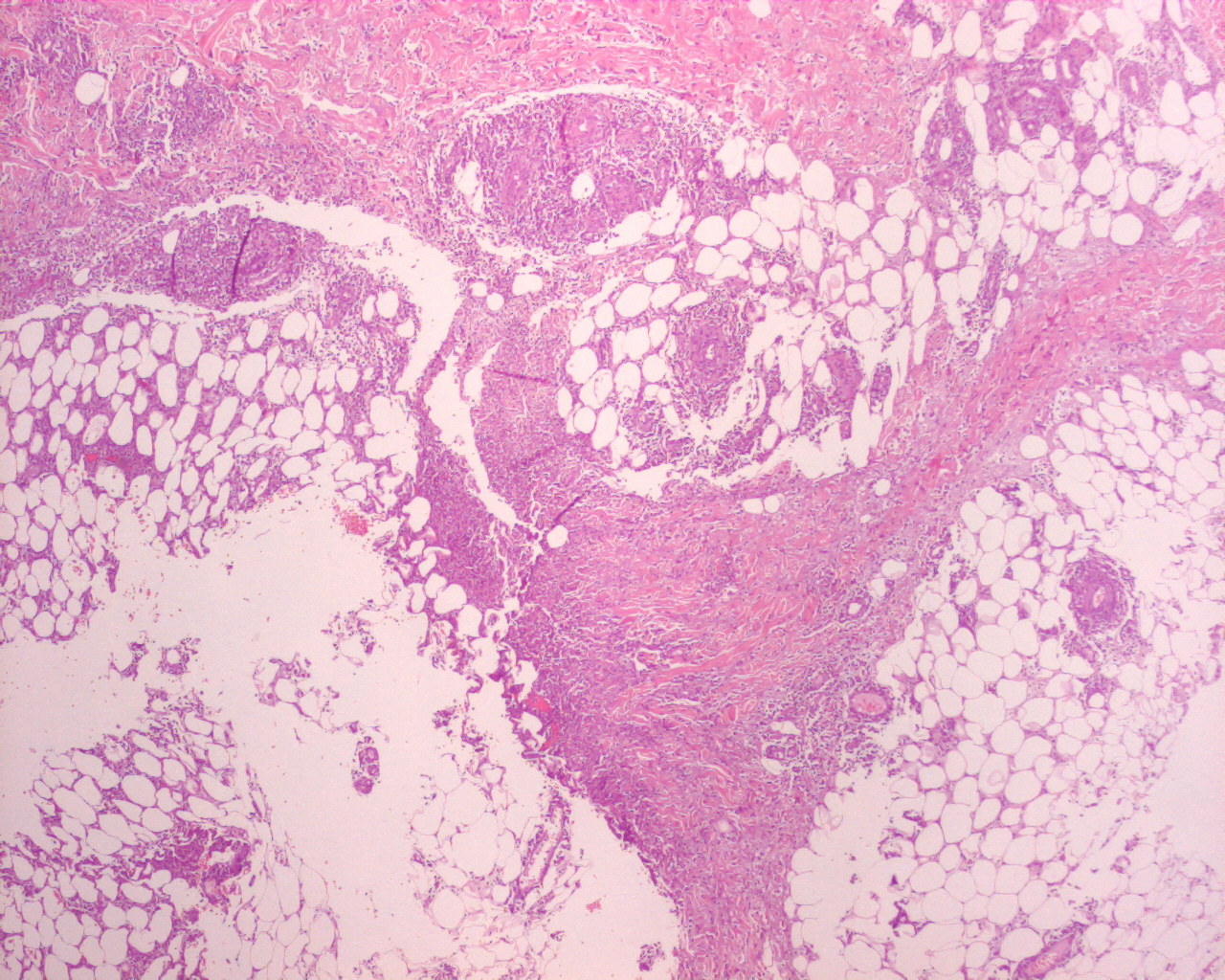
| Figure 10. Histopathologic examination of a skin biopsy from an erythema-nodosum-like nodules shows a normal epidermis and
lymphocytic vasculitis in the dermis (H&E x4) Figure 11. Histopathologic features show the coexistence of lymphocytic vasculitis and mixed panniculitis (H&E x4) | |
 |  |
| Figure 12 | Figure 13 |
|---|---|
| Figure 12. Higher amplification of the same cutaneous lesions (H&E x20) Figure 13. Inflammatory infiltrate extends to the adnexal structures (H&E x20) | |
Histopathologic examination of a skin biopsy from an erythema nodosum-like nodule showed a normal epidermis, lymphocytic vasculitis in the dermis, and a mixed panniculitis with an inflammatory infiltrate extending to the adnexal structures at the dermo-hypodermal junction. Pathergy test was negative. Ophthalmologic examination detected papilledema. Cerebral MRI and lumbar puncture revealed features of rhombencephalitis. HLA-B51 was positive. Altogether, these findings allowed the diagnosis of Behçet disease and the patient started a 3-day course of pulse iv methylprednisolone 1g qd, followed by oral prednisone, 1 mg/kg/day, without any improvement.
 |  |
| Figure 14 | Figure 15 |
|---|---|
| Figure 14. Complete resolution of the aphthous ulcer on the upper lip after a single infusion of infliximab Figure 15. Clearance of the cutaneous lesions in the thorax and abdomen with treatment | |
 |  |
| Figure 16 | Figure 17 |
|---|---|
| Figure 16. Resolution of the cutaneous lesions on the back Figure 17. Complete clearing of the erythema nodosum-like nodules on the lower limbs after infliximab therapy | |
For this reason, she started IV infliximab 5 mg/kg every 6 weeks with complete resolution of clinical disease after the first infusion and without sequelae. The patient remains free of the disease after one year of follow-up, still under infliximab therapy.
Discussion
Behçet disease is a chronic systemic inflammatory disorder of unknown etiology. The exuberant and sudden onset of the multi-systemic involvement in our patient is uncommon and usually related with a poor prognosis [1, 2]. Along with this severe presentation, the presence of HLA-B51 and the lack of response to high-dose corticosteroids were also predictive of a worse outcome [1, 2, 3]. Such a dramatic clinical picture requires aggressive immunosuppressive therapy in order to achieve rapid control of the disease and avoid irreversible damage to vital organs [1, 2, 3]. Anti-TNFα agents have been used in Behçet disease because of a role of TNFα mediated interactions in its pathogenesis [1, 4]. Among these agents, there is greater information on infliximab; 83 percent of Behçet disease patients on anti-TNFα agents are receiving infliximab [1-3, 5, 6]. This fact, along with the documented high efficacy rates (>85%) and the rapid effect after a single infusion make it a good candidate for severe presentations resistant to standard therapies or for those intolerant to those treatments [1-6]. For these reasons, we started infliximab in our patient and obtained a rapid and complete response. Since relapses are not uncommon after cessation of the anti-TNFα treatment [1, 2, 3], the patient has been kept on the same therapeutic regimen, so far without complications after 1 year of follow-up. In summary, there is sufficient scientific evidence to support the use of infliximab in severe, refractory cases of Behçet disease. At the same time we must keep in mind that this entity has a chronic course, with successive remissions and relapses, highlighting the importance of a long-term effective and safe therapy. Because there are no data regarding the efficacy and safety of infliximab in Behcet disease over the long term, future studies are needed in order to optimize treatment protocols and clarify the role of anti-TNFα agents.
References
1. Aikaterini A, Fragiadaki K, Giavri E, Sfikakis PP. Anti-TNF agents for Behçet’s disease: analysis of published data on 369 patients. Semin Arthritis Rheum. 2011 Aug;41(1):61-70. [PubMed]2. Zaidan M, Lidove O, Sacré K, Klein I, Papo T. “Fulminant” Behçet disease. Presse Med. 2011 Nov;40(11):1087-9. [PubMed]
3. Lestre S, Trindade F, Martins A, Baptista J, Feio AB, Lopes MJ. Behçet’s disease - Infliximab in the treatment of mucocutaneous manifestations. Acta Reumatol Port. 2009 Oct-Dec;34(4):633-40. [PubMed]
4. Sugita S, Yamada Y, Kaneko S, Horie S, Mochizuki M. Induction of regulatory T cells by infliximab in Behcet’s disease. Invest Ophthalmol Vis Sci. 2011 Jan 21;52(1):476-84. [PubMed]
5. Borhani Haghighi A, Safari A, Nazarinia MA, Habibagahi Z, Shenavandeh S. Infliximab for patients with neuro-Behcet’s disease: case series and literature review. Clin Rheumatol. 2011 Jul;30(7):1007-12. [PubMed]
6. Abalos-Medina GM, Sánchez-Cano D, Ruiz-Villaverde G, Ruiz-Villaverde R, Quirosa Flores S, Raya Alvarez E. Successful use of infliximab in a patient with neuro-Behçet's disease. Int J Rheum Dis. 2009 Sep;12(3):264-6. [PubMed]
© 2013 Dermatology Online Journal