Reticulate acropigmentation of Kitamura: Report of a familial case
Published Web Location
https://doi.org/10.5070/D36ss0523mMain Content
Reticulate acropigmentation of Kitamura: Report of a familial case
Emek Kocatürk MD1, Mukaddes Kavala MD1, Ilkin Zindanci MD1, Ebru Zemheri MD1, Melek Kesir Koç MD1, Sükran Sarigül MD2
Dermatology Online Journal 14 (8): 7
1. Goztepe Training and Resarch Hospital, Department of Dermatology, Istanbul, Turkey. emekozgur@yahoo.com2. Fatih Sultan Mehmet Training and Research Hospital, Department of Dermatology, Istanbul, Turkey
Abstract
Reticulate Acropigmentation of Kitamura (RAPK) was first described in Japan and most cases reported have been in patients of Asian ethnic groups. Angulated, slightly atrophic, hyperpigmented macules that are arranged in a reticulate pattern are typically found on the dorsal hands and feet. The condition is inherited in an autosomal dominant fashion and skin changes begin to develop during childhood. We report RAPK in a mother and daughter who are from a non-Asian ethnic group.
Case 1
 |  |
| Figure 1 | Figure 2 |
|---|
A 53-year-old woman was referred to our clinic because of pigmentation involving the flexural areas. The pigmentation started on the hands and feet while she was in her twenties, progressed to the flexural areas, and darkened. Her familial history is significant in that her grandmother, mother and her two daughters also had similar freckle-like pigmentation on the hands, feet and in flexural areas. Her medical history was significant for skin and lung sarcoidosis that had been treated with systemic corticosteroids. Dermatological examination revealed punctate, irregular, slightly atrophic, brown macules involving the dorsa of the hands and feet, the extensor surface of the neck, both axillary regions, the inguinal region, the dorsa of the knees and the abdominal skin (Figs. 1 & 2). In addition, irregular breaks in the dermatoglyphics on the thenar and hypothenar regions of the palms were noticed (Fig. 3).
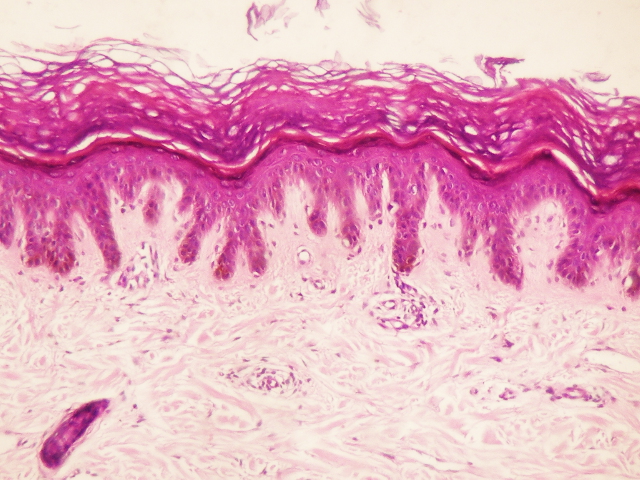
A skin biopsy taken from the dorsa of the knee revealed hyperkeratosis, thinning of the epithelium, filiform elongation of the rete ridges and sparse lymphocyte infiltration at the dermis (Fig. 4). Based on the clinical and histological findings she was diagnosed as reticulate acropigmentation of Kitamura (RAPK).
 |  |
| Figure 3 | Figure 4 |
|---|
Case 2
 |
| Figure 5 |
|---|
The daughter of Case 1, who was a 32-year-old woman, had a history of similar lesions which also started while she was in her twenties. She was otherwise healthy. On examination, she had irregular, atrophic, freckle-like macules on the neck, elbows, abdominal skin, and dorsa of the hands and feet (Fig. 5). It was noted that the freckle-like lesions were not as dark as in the mother.
Discussion
RAPK was first described in Japan: about 100 cases have been reported, mostly in Asian ethnic groups. Most of these cases involve patients with dark or black skin, including people from India, Turkey, Iran, Saudi arabia, Italy and Latin America [1].
The characteristic presentation of RAPK is as pigmented, angulated, irregular freckle-like lesions with atrophy on the surface, arranged in a reticular pattern on the dorsa of the hands and feet. The lesions usually start in the first and second decades of life and gradually extend onto the extremities and rarely on the face and eyelids. The lesions usually slowly darken over time [2]. Sunlight may aggrevate the condition. Pits and breaks in the dermatoglyphics are found on the palms, soles and dorsal phalangeal surfaces [3].
Histopathological examination classically shows epidermal atrophy associated with club-like elongation of the rete ridges and an excess of melanin in the basal layer [1].
The differential diagnosis of RAPK include diseases presenting with reticulated or punctate hyperpigmentation like dyskeratosis congenita, dyschromatosis universalis herediteria, Franceschetti-Jadassohn's syndrome, dermatopathia pigmentosa reticularis, acropigmentation of Dohi (RAD) and Dowling-Degos Disease (DDD) [4]. RAD is also an acral type of dyschromatosis (dyschromatosis symmetrica herediteria) that usually starts in infancy or early childhood as hypopigmented and hyperpigmented macules over the dorsa of the hands and feet. The differentiation between RAD and RAPK is based on clinical and histological findings. In RAPK there are usually no hypopigmented macules and histologically there is epidermal atrophy and increase in the number of basal melanocytes. DDD is also an autosomal dominant pigmented skin disorder characterized by reticular hyperpigmentation on flexor areas such as the neck, axilla, antecubital fossa, submammary area and groin. Dark comedo-like lesions and pitted perioral acneiform scars may be present. Rarely hypopigmented macules or papules are observed. Histologically there are pigmented filiform epidermal projections involving the follicular infundibulum as well as the epidermis [5, 6].
Recently there have been increasing reports on the coexistence of RAPK and Dowling Degos Disease in the same patient. Therefore some authors suggest that RAPK and DDD are different ends of the spectrum of the same disease. In 1986, Crovato reported a family in which the clinical features of Dowling Degos disease were associated with those of RAPK [7]. But since genes for these pigmentary disorders have not been mapped, it is hard to prove these associations.
Most treatments attempted have been unsuccessful, but an attempt to treat the disease with 20 percent azelaic acid gave significant improvement [3]. Our patients did not agree to any treatment.
These cases have a significance for reminding us that although RAPK is a common disease in Asian populations, we must keep in mind that we may also encounter this disease in different parts of the world.
References
1. Bolognia JL, Jorizzo LJ, Rapini RP in Dermatology. Chang MW.Pigmentary Disorders. Second Ed, Elsevier, USA. 939-663.2. Sharma R, Sharma SC, Radotra BD, Kaur S. Reticulate acropigmentation of Kitamura. Clin Exp Dermatol. 1989 Jul;14(4):302-3. PubMed
3. Kameyama K, Morita M, Sugaya K, Nishiyama S, Hearing VJ. Treatment of reticulate acropigmentation of Kitamura with azelaic acid. An immunohistochemical and electron microscopic study.J Am Acad Dermatol. 1992 May;26(5 Pt 2):817-20. PubMed
4. Ays¸in Köktürk, Güliz I˙kizog˘lu, Kıymet Baz, Tamer I˙rfan Kaya. Kitamura’nın Retiküler Akropigmentasyonu ve Dowling-Degos Hastalığı özelliklerini taşıyan bir olgu. TÜRKDERM 2002;36:286-289.
5. Alfadley A, Al Ajlan A, Hainau B, Pedersen KT, Al Hoqail I. Reticulate acropigmentation of Dohi: a case report of autosomal recessive inheritance. J Am Acad Dermatol. 2000 Jul;43(1 Pt 1):113-7. PubMed
6. Wu YH, Lin YC. Generalized Dowling-Degos disease. J Am Acad Dermatol. 2007 Aug;57(2):327-34. PubMed
7. Crovato F, Rebora A: Reticulated pigmented anomaly of the flexures associating reticulate acropigmentation: One single entity. J Am Acad Dermatol 1986;14:359-361. PubMed
© 2008 Dermatology Online Journal