Seborrheic keratosis with in-situ squamous cell carcinoma changes
Published Web Location
https://doi.org/10.5070/D37nt5n5m9Main Content
Seborrheic keratosis with in-situ squamous cell carcinoma changes
Poonam Sharma MD, Deba P Sarma MD, Edward D Adickes DO
Dermatology Online Journal 12 (7): 19
Department of Pathology, Creighton University Medical Center, Omaha Nebraska. dpsarma@yahoo.com
We are reporting a rare case of seborrheic keratosis with Bowenoid changes occurring in an 80-year-old man. The English literature on the topic is briefly reviewed.
Clinical synopsis
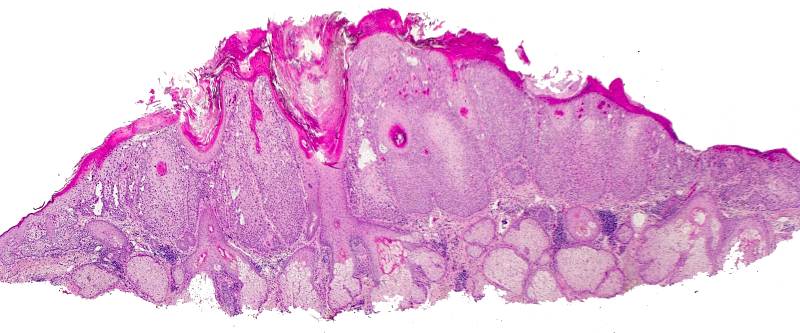
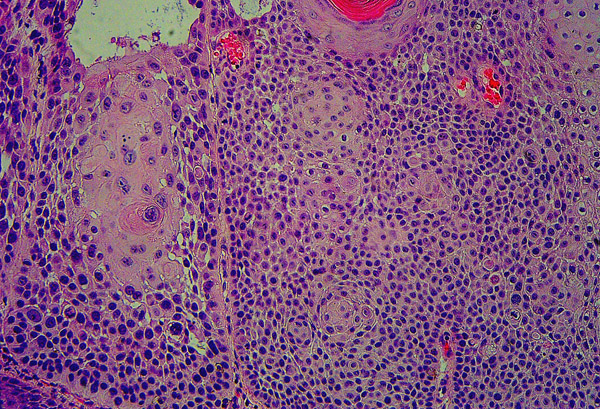
An 80-year-old man presented with a long-standing skin lesion on his mid forehead, clinically thought to be squamous cell carcinoma. An excisional biopsy was performed. The specimen consisted of a rounded piece of skin measuring 0.8 cm in maximum dimension that featured a raised verruciform epidermal lesion. Microscopic examination revealed a raised stuck-on epidermal neoplasm showing basaloid dark epidermal cells over the deep part of the lesion. There were several benign squamous eddies suggesting irritated pattern of seborrheic keratosis. A few horn cysts were noted. The superficial part of the lesion showed papillomatosis and hyperkeratosis (Fig. 1). The benign basaloid squamous cells gradually blended with areas of markedly dysplastic squamous cells with numerous mitoses in a disorderly growth pattern, indicative of in-situ carcinoma. The entire lesion also showed areas of acantholysis (Fig. 2).
|
|
| Figure 1 | Figure 2 |
|---|---|
|
Figure 1. Low magnification showing seborrheic keratosis (magnification X 4) Figure 2. High magnification shows seborrheic keratosis with several squamous eddies on the right side and dysplastic pleomorphic squamous cells of in-situ carcinoma on the left side (magnification X 40) |
|
Comment
Seborrheic keratosis is a common benign epidermal neoplasm occurring in about 20 percent of the elderly population. Malignant transformation of such a tumor is a very rare event. Sloan and Jaworsky noted 60 cases of in-situ squamous cell carcinoma occurring among 4310 cases (1.4 %) of clinically diagnosed seborrheic keratosis [1]. Malignant change seems to occur in the lesions located in the head and neck, typically exposed to solar degeneration. In addition to in-situ squamous cell carcinoma, invasive squamous cell carcinoma and basal cell carcinoma arising in seborrheic keratosis have been reported [2, 3]. Malignant change, mostly in-situ carcinoma, is usually detected on the microscopic examination of a long-standing seborrheic keratosis located in the head and neck, and with a recent history of ulceration or increasing size. Many of these cases are probably histologically interpreted as an in-situ carcinoma because the residual seborrheic keratosis may be difficult to detect.
References
1. Sloan JB, Jaworsky C. Clinical misdiagnosis of squamous cell carcinoma in situ as seborrheic keratosis. A prospective study. J Dermatol Surg Oncol 1993; 19:413-416.2. Yap WM, Tan PH, Ong BH. Malignancy arising in seborrheic keratosis: a report of two cases. Ann Acad Med Singapore 1997; 26:235-237.
3. Kwittken J. Malignant changes in seborrheic keratosis. Mt Sinai J Med 1974; 41:792-801.
© 2006 Dermatology Online Journal